At the Centeno-Schultz Clinic we approach pain and dysfunction in a systematic fashion which is outlined in Ortho 2.0.
We employ the acronym SANS: symmetry, articulation, neurologic and stability.
This approach can be utilized for any joint.
The iliotibial band (ITB) is a fibrous band that extends from the hip (ilium) to the knee (tibia).
It is a critical in the stability of the hip and pelvis.
There are both anterior and posterior forces on the ITB.
Posteriorly it connects with the gluteus medius muscle which when contracted pulls the ITB posteriorly.
Anteriorly the ITB connects with the tensor fasciae latae muscle which when contracted pulls the ITB anteriorly.

Biomechanics of ITB: Supports and stabilizes the hip and pelvis when the opposite foot is suspended and off the floor such as when we are walking.
Lumbar spinal nerves provide essential information to the gluteus medius, tensor fasciae latae and other muscles that support the ITB.
Irritation or compression of lumbar nerves can result in a reduction in the nerve signal to the muscles and ensuing weakness.
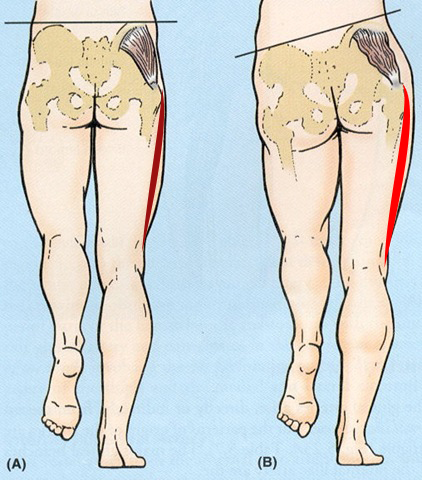
This weakness can be witnessed on physical examination when the patient is asked to stand on one leg and the pelvis shifts. Weakness in the ITB compromises the stability of the pelvis and hip with resultant shift of the pelvis as illustrated below.
An excellent analysis and summary of the iliotibial band is presented below by Dr. Centeno.


